The following are scenarios where patients may have been exposed to rabies. Each situation is distinct, and an appropriate treatment approach requires a clear understanding of post-exposure prophylaxis (PEP) guidelines and options available.
Select from the scenarios below to guide you to each individual profile.
Spencer, age 12

Potential Rabies Exposure:
While playing at a park with friends, Spencer went into a wooded area to retrieve a lost ball and encountered an aggressive raccoon. The animal attacked and Spencer fended it off by repeatedly kicking at it. Spencer, who had been wearing shorts, was left with multiple scratches on his right leg. A friend’s father brought Spencer to the ER.
Treatment scenario for this teen weighing 89 lb/40.4 kg:
Rabies PEP was administered based on the patient’s age and weight. The full dose of HRIG (5.4 mL) was administered carefully into and around all detectable wounds. A rabies vaccine was then injected intramuscularly into the deltoid muscle.
Weight: 89 lb/40.4 kg
Animal exposure: Raccoon
Wounds location: Right leg
Anton, 11 months

Potential Rabies Exposure:
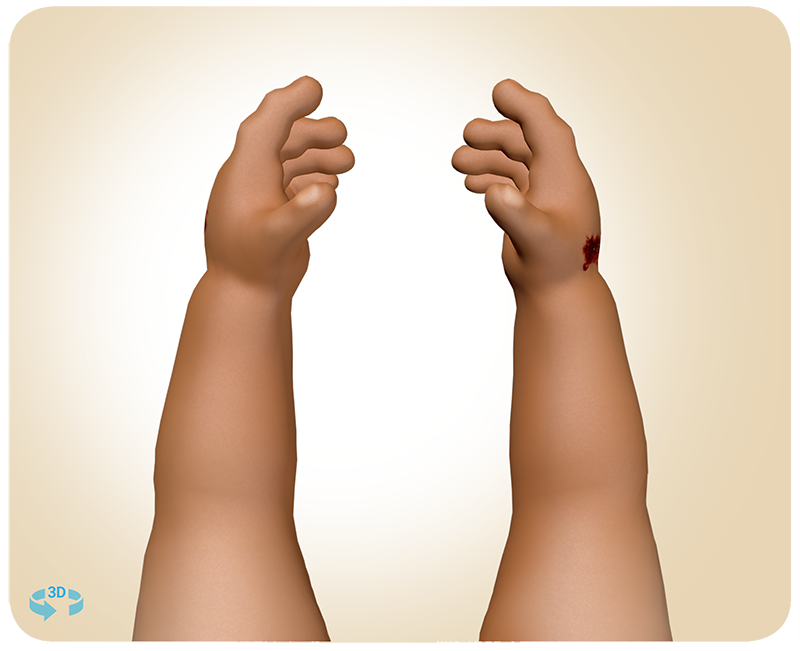
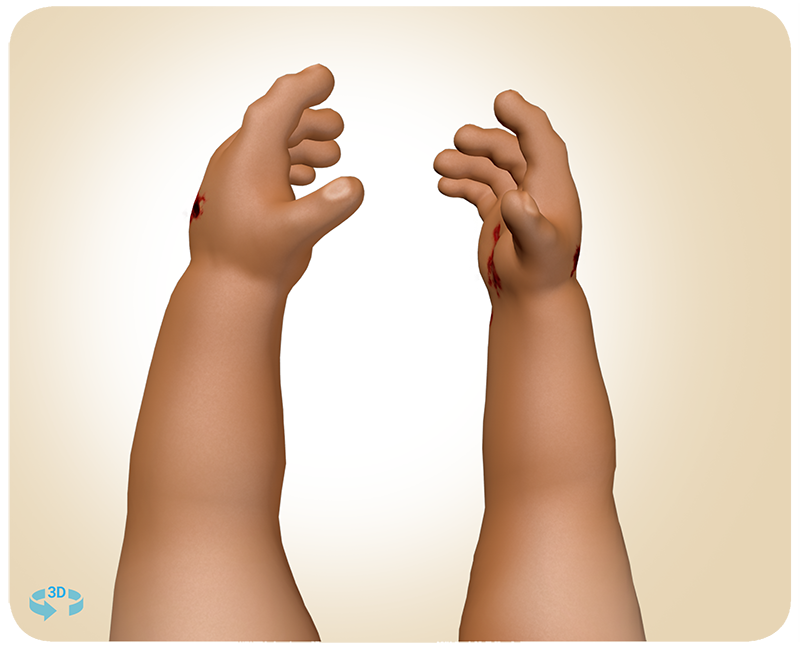
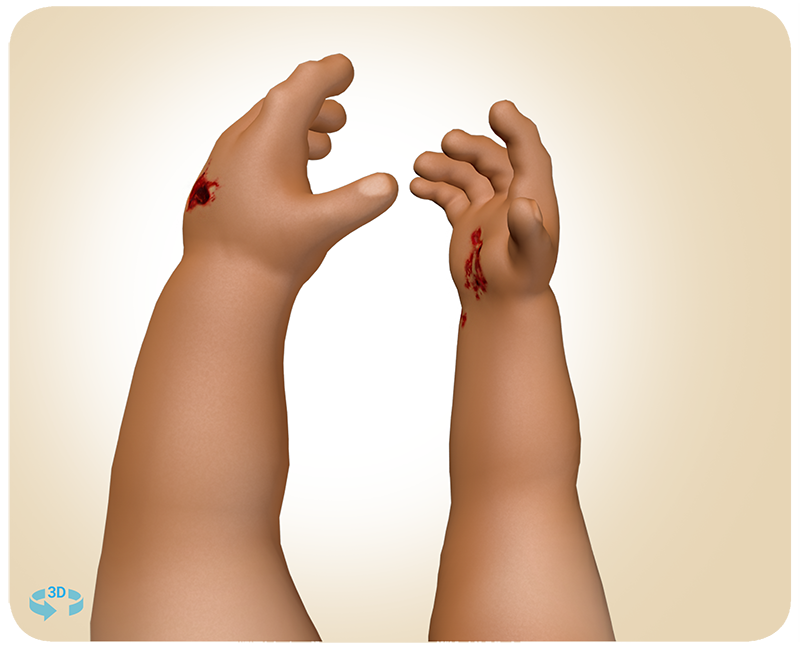
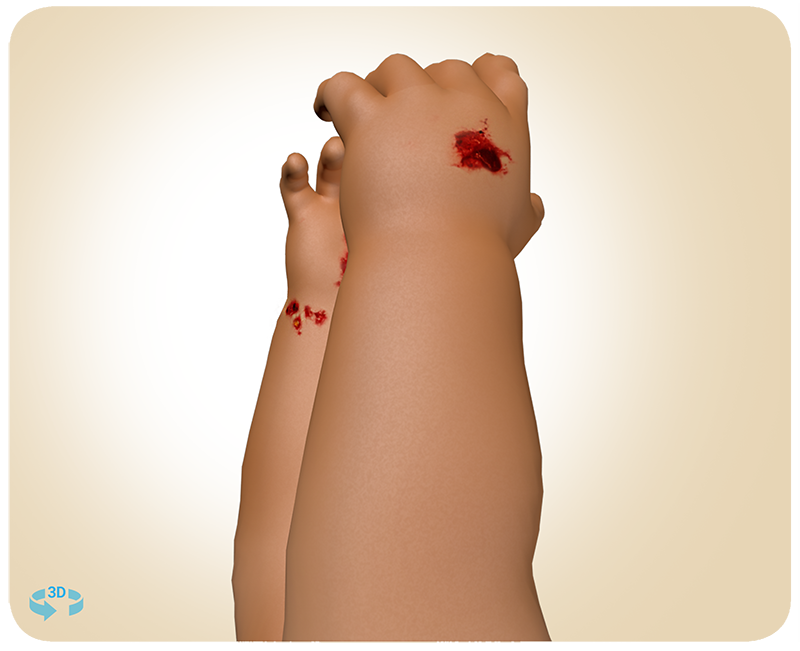
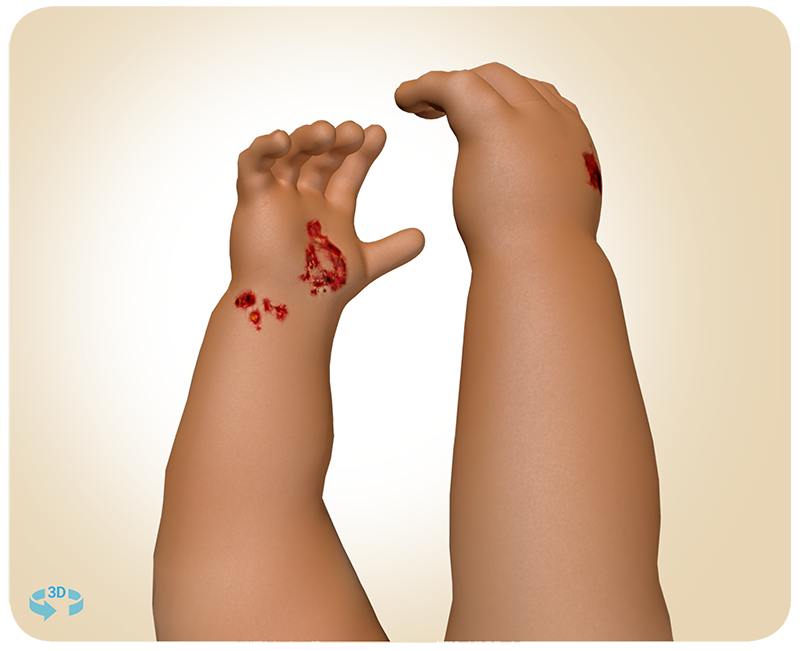
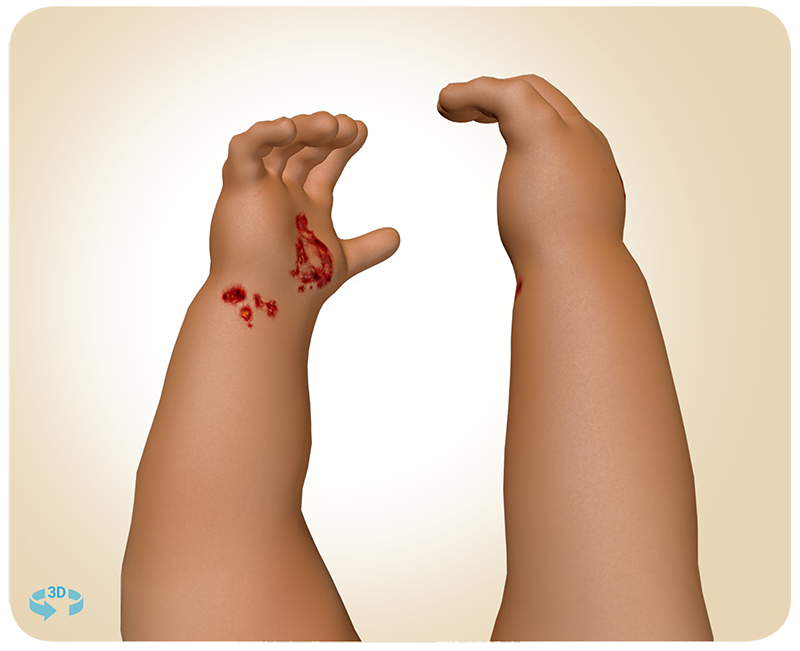
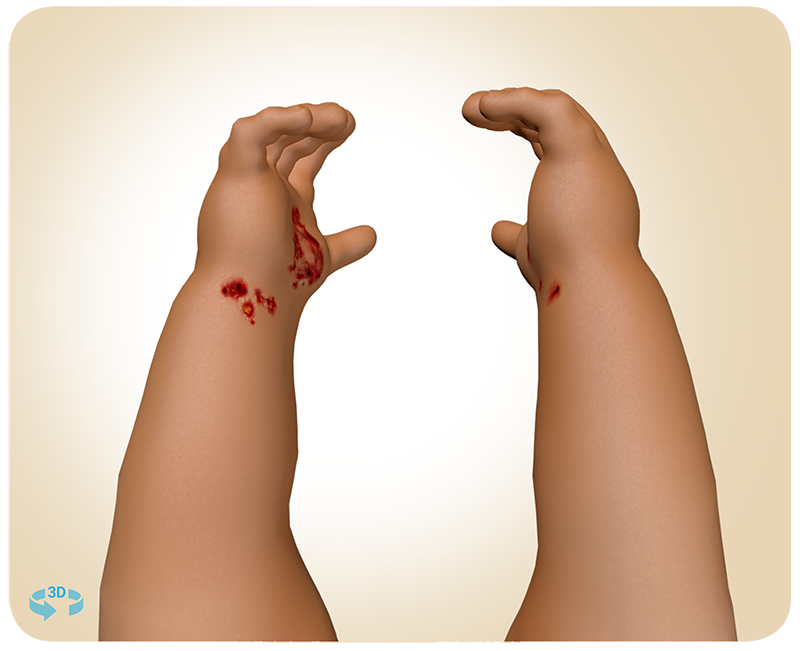
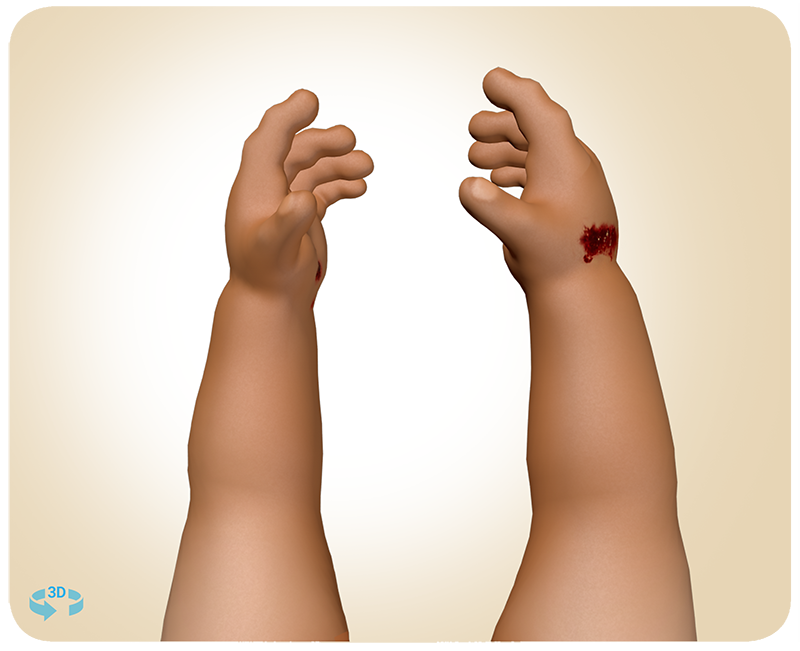
A grandmother was babysitting her 11-month old grandson. While playing in the front yard, an unleashed dog came running over. Playful at first, it then aggressively pushed over the boy and bit him on both hands. Shocked, the grandmother called for an ambulance and they went to the ER. It was unknown if the dog had previously received a rabies vaccine series.
Treatment scenario for this baby weighing 20 lb/9.1 kg:
Rabies PEP was administered (1.2 mL HRIG dose) based on the patient’s age and weight. Since the patient was young with low body weight – extra caution was taken to identify an appropriate HRIG product, with enough dose volume to properly infiltrate all wounds.
Weight: 20 lb/9.1 kg
Animal exposure: Dog
Wounds location: Hands
Cassie, age 26
Potential Rabies Exposure:
Cassie was staying at a friend’s family vacation home and slept in a converted attic bedroom space. She woke early in the morning to the sound of something fluttering near the ceiling, but couldn’t see what it was. She then noticed 4-5 very small bite marks on her hand. After speaking to her friend’s family at breakfast, they decided to go to the ER to be safe.
Treatment scenario for this adult weighing 140 lb/63.5 kg:
Rabies PEP was administered (8.5 mL HRIG dose) based on the patient’s weight. HRIG was infiltrated thoroughly into and around all visible wounds and the remaining volume from the 8.5 mL HRIG dose was given by the intramuscular route at a site distant from the site of the rabies vaccination.
Weight: 140 lb/63.5 kg
Animal exposure: Bat
Wounds location: Hand
Improper HRIG Administration Can Lessen the Effect of a Rabies Vaccine
Because HRIG can partially suppress active production of rabies virus antibodies, no more than the recommended dose should be administered.1
Is the Volume of Your HRIG Dose Adequate for Treating All Rabies Exposures?
Ready-to-Use KEDRAB® (Rabies Immune Globulin [Human]) at 150 IU/mL Potency Ensures You Have1:
- The appropriate volume needed to treat any rabies exposure1
- No need for dilution with dextrose, which may help reduce the potential for errors caused by the need to prepare an admixture1,2
Does a Higher Volume Increase the Chance for Compartment Syndrome?
In a prospective study involving 100 high-risk HRIG injections (fingers and toes) during proper PEP protocol, no case of compartment syndrome was found. In researching data from the past two decades, where HRIG was administered to patients potentially exposed to the rabies virus, no cases of compartment syndrome were found by the study authors.3

View additional HRIG administration scenarios highlighting different vectors and wound sizes
References: 1. KEDRAB [package insert]. Fort Lee, NJ: Kedrion Biopharma Inc.; 2021. 2. Billstein-Leber M, Carrillo CJD, Cassano AT, Moline K, Robertson JJ. ASHP Guidelines on Preventing Medication Errors in Hospitals. Am J Health Syst Pharm. 2018;75:1493-1517. doi:10.2146/ajhp170811. 3. Shantavasinkul P, Wilde H. Postexposure prophylaxis for rabies in resource-limited/poor countries. Adv Virus Res. 2011;79:291-307.